| gence of the modern state with its agencies for collecting
information on its citizens and their activities, and the theoretical interest
of political economists in finding causes for human social behaviors. These
three movements, Walker wrote, were pulled together in the career of
the mid-l9th-century Belgian astronomer-statistician Lambert-Adolphe-Jacques
Quételet, widely regarded as the founder of modern social statistics.
In 1841 Quételet organized Belgiums central statistical bureau,
which became a model for similar agencies in other countries, and his international
leadership in statistical research continued until his death in 1874.
Nineteenth-century
scholars trying to make a science out of the study of human behavior faced
a dilemma: the model science of those days was classical physics, with
its deterministic laws describing natural phenomena, but human behavior
seemed individual and indeterminate. Quételets resolution of the
problem bypassed the question of the individual with the concept of an
average man. He showed that whereas there are no laws determining individual
behavior, there are regularities in the attributes and behavior of groups,
and that these regularities could be characterized mathematically by the
laws of probability. Quételet was convinced that even menial and
moral traits, if only they could be measured accurately, would also follow
regular laws of statistical distribution.
Quételets most original
and most startling work was his analysis of the influence of such factors
as sex, age, education, climate and season on the French crime rate (1831).
The data did not allow a prediction of who would commit what crime, but
according to Quételet they did display regularities that would enable
a scientist to enumerate in advance how many individuals will stain their
hands in the blood of their fellows, how many will be forgers, how many
will be poisoners. The discovery of these regularities led Quételet
to the radical conclusion that it is sociely which, in some way, prepares
these crimes, and the criminal is only the instrument that executes them.
Although Quételets work
was highly regarded by many scholars, it was abhorred by others. The determinism
of his social physics was an anathema to people committed to the prevailing
doctrines of free will and individual responsibility. John Stuart Mill,
for example, wrote at length against probability in general and its application
to social science in particular. Another vocal opponent of the statistical
view of man and society was Charles Dickens. His novel Hard Times
was meant to satirize those people, Dickens later said, who could see nothing
but figures and averages,
133 |
those addled heads who would use the yearly average
temperature in the Crimea as a reason for clothing a soldier in nankeens
[silks] on a night when he would be frozen to death in fur. Dickens disliked
the statistical view because he thought it was dehumanizing, and in Hard
Times he portrayed the regularities found by statisticians in the rate
of insanity, crime, suicide and prostitution as a deadly statistical clock.
Nightingale, on the other hand,
was an ardent admirer of Quételets work, and she early displayed
a predilection for collecting and analyzing data. At Scutari,
apart from the all-important sanitary reforms she instituted, she also
systematized the chaotic reord-keeping practices; until then even the number
of deaths was not known with accuracy. When she returned to England in
1856, she met William Farr, a physician and professional statistician.
Under Farrs guidance Nightingale soon recognized the potential of the
statistics she had gathered at Scutari, and of medical statistics in general,
as a tool for improving medical care in military and civilian hospitals.
Throughout ut military history until
the 20th century the main cause of death in war was disease rather than
wounds sustained in battle, and the Crimean War was no exception. Nightingales
numbers still speak eloquently. During the first months of the Crimean
campaign there was a mortality among the troops at the rate of 60 percent
per annum from disease alone, a rate exceeding that of the Great Plague
of 1665 in London and higher also than the mortality in cholera to the
attacks (that is, the mortality among those who had contracted the disease).
In January, 1855, the mortality in all British hospitals in Turkey and
the Crimea, measured in relation to the entire army in the Crimea but not
including men killed in action, peaked at an annual rate of 1,174 per 1,000.
Of this number 1,023 deaths per 1,000 were attributable to zymotic disease
(a category introduced by Farr including epidemic, endemic and contagious
disease). This means that if mortality had persisted for a full year at
the rate that applied in January, and if the dead soldiers had not been
replaced, disease alone would have wiped out the entire British army in
the Crimea.
Nightingales various methods
of calculating mortality dramatized both the impact of disease and the
effects of improved sanitary conditions. Calculated on an annual basis
as a percentage of the patient population, the death rate at the Scutari
hospital reached an incredible 415 percent in February, 1855. In March,
however, Nightingales sanitary reforms began to be implemented and mortality
among the patients declined precipitously. By the end of the war, according
to Nightingale, the |
death rate among sick British soldiers in Turkey
was not much more than it was among healthy soldiers in England; even
more remarkable, the mortality among all British troops in the Crimea was
two-thirds only of what it [was] among our troops at home.
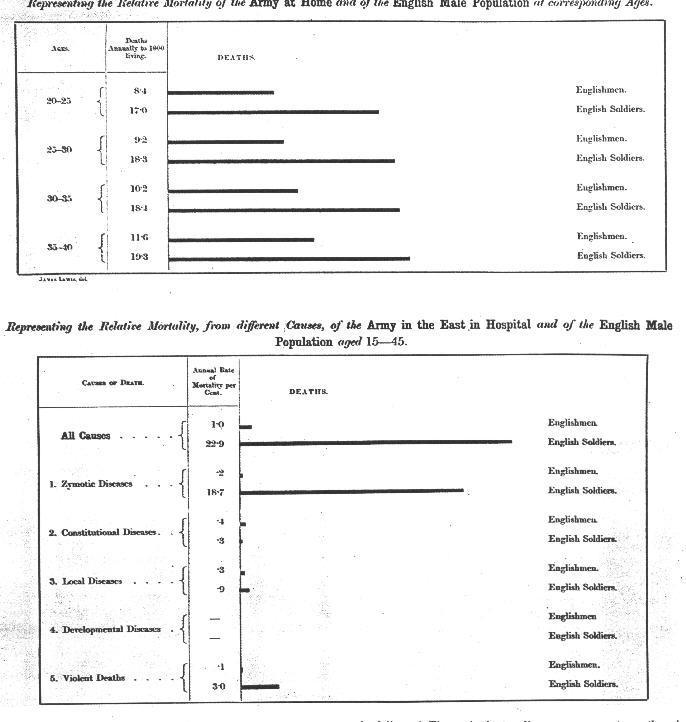
The comparison suggested that
the soldiers at home were living in their barracks under unhealthy conditions.
After Farr had made Nightingale aware of the significance of mortality
tables, she at once thought of comparing the mortality among civilians
to that among soldiers. She found that in peacetime soldiers in England
between the ages of 20 and 35 had a mortality rate nearly twice that of
civilians. It is just as criminal, she wrote in 1857, to have a mortality
of 17, 19, and 20 per thousand in the Line, Artillery and Guards in England,
when that of Civil life is only 11 per 1,000, as it would be to take 1,100
men per annum out upon Salisbury Plain and shoot them. (The 1,100 represented
20 per 1,000 of an enlisted force of 55,000.) Clearly the need for sanitary
improvements in the military was not limited to hospitals in the field.
By pressing her case with these statistics Nightingale eventually gained
the attention of Queen Victoria and Prince Albert, as well as of the prime
minister, Lord Palmerston. In spite of the passive resistance of the War
Office, Nightingales wish for a formal investigation of military health
care was granted in May, 1857, with the establishment of a Royal Commission
on the Health of the Army.
It would not have been possible
at that time for a woman to serve on such a board. Nightingale nonetheless
strongly influenced the commissions work, both because some of its members
were her friends (including Sidney Herbert, the minister who sent her to
the Crimea) and because she provided it with much of its information. As
a statement of her own views she wrote and had privately printed an 800-page
book titled Notes on Matters Affecting the Health, Efficiency and Hospital
Administration of the British Army, which included a section of statistics
accompanied by diagrams. Farr called it the best [thing] that ever was
written either on statistical Diagrams or on the Army.
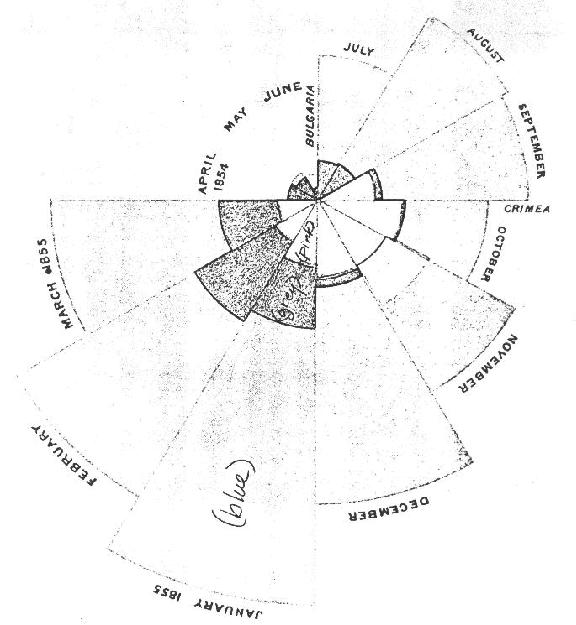
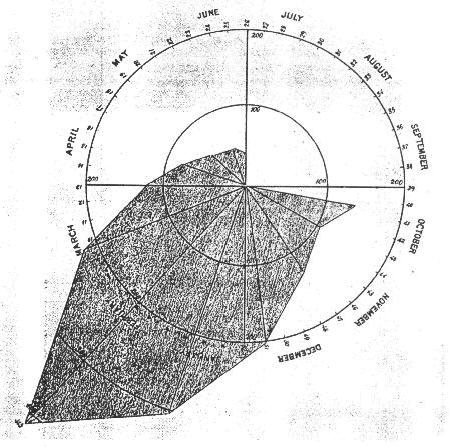
Nightingale was a true pioneer
in the graphical re presentation of statistics: she invented polar-area
charts, in which the statistic being represented is proportional to the
area of a wedge in a circular diagram. Nightingale used these diagrams,
which she called her coxcombs because of their vivid colors, to dramatize
the extent to which deaths in the Crimea campaign had been preventable.
Farr was impressed with Notes, and much of Nightingales work found
its way into the statistical charts and diagrams he prepared for the final
report of |